 Precision oncology is transforming cancer care by shifting from traditional trial-and-error treatments to personalized therapies based on each patient’s unique molecular profile. By leveraging advanced biomarkers, genomic insights, and targeted treatments, modern oncology aims to improve outcomes while reducing unnecessary toxicity and enhancing quality of life.
Precision oncology is transforming cancer care by shifting from traditional trial-and-error treatments to personalized therapies based on each patient’s unique molecular profile. By leveraging advanced biomarkers, genomic insights, and targeted treatments, modern oncology aims to improve outcomes while reducing unnecessary toxicity and enhancing quality of life.




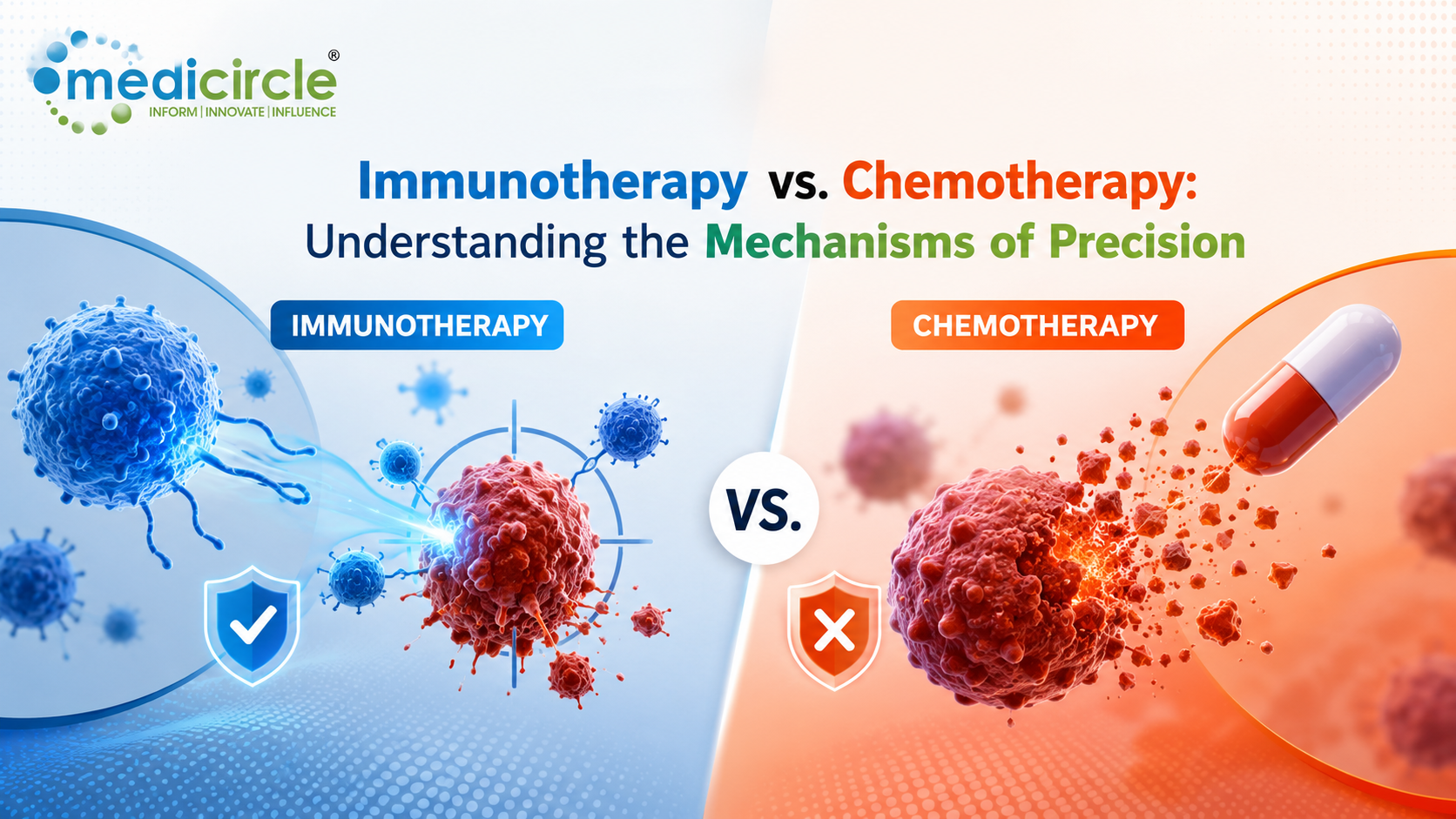
The global oncology landscape is undergoing a revolutionary transformation. For decades, the therapeutic roadmap for managing advanced malignancies relied almost exclusively on a rigid trial-and-error framework. However, clinical oncology has fundamentally pivoted toward precision medicine—using patient-specific biomolecular profiles to design highly individualized therapies that maximize cellular efficacy while minimizing systemic toxicity.
At the center of this transformation is the structural shift from conventional chemotherapy to advanced immunotherapy. While both modalities remain primary pillars of the oncological arsenal, their mechanical blueprints, cellular targets, and long-term physiological footprints represent completely distinct strategies.
Understanding the differences between these two forces requires looking past generic product branding to evaluate the precise cellular and immunological mechanics that dictate modern patient care.
1. The Direct Assault: Cytotoxic Chemotherapy Mechanics
Chemotherapy functions as a direct, systemic chemical assault. Rather than identifying individual cancer cells by their unique genetic mutations or surface receptors, conventional chemotherapy exploits a hallmark characteristic of all malignant tissues: rapid, uncontrolled cellular division (mitosis).
[ THE CYTOTOXIC CHEMOTHERAPY MECHANISM ]
│
┌────────────────────────┴────────────────────────┐
▼ ▼
[ DNA REPLICATION BLOCK ] [ MITOTIC SPINDLE ARREST ]
• Alkylating agents cross-link DNA strands • Taxanes freeze microtubule disassembly
• Antimetabolites fool replication machinery • Vinca alkaloids block spindle formation
• DNA synthesis fails; apoptosis triggers • Mitosis collapses; rapid cell death
Chemotherapy drugs are engineered to disrupt the cell lifecycle at specific operational checkpoints:
- DNA Replication Inhibitors: Alkylating agents introduce covalent bonds into DNA bases, forming structural cross-links that prevent the double helix from unwinding. Antimetabolites masquerade as natural nucleotides, tricking the cell into incorporating faulty bases into its expanding DNA strand. These disruptions halt DNA synthesis, triggering automated intracellular emergency signals that force apoptosis (programmed cell death).
- Mitotic Spindle Arrestors: Microtubule-targeting agents, such as taxanes and vinca alkaloids, attack the physical scaffolding responsible for pulling duplicated chromosomes apart during cell division. Taxanes hyper-stabilize these microscopic tubes, freezing them in place, while vinca alkaloids suppress their formation entirely. Deprived of functioning mitotic spindles, the dividing cell collapses and degrades.
Because chemotherapy targets the mechanism of cell replication rather than a specific cancer marker, it cannot differentiate between a malignant tumor and high-turnover healthy tissue. Systemic side effects—such as bone marrow suppression (leading to dropped white blood cell counts and severe fatigue), gastrointestinal lining degradation (causing acute nausea), and hair follicle cell death—are the direct consequence of this broad cellular attack.
2. Unmasking the Enemy: Precision Immunotherapy Mechanics
Immunotherapy represents an entirely different strategic philosophy. Instead of introducing an exogenous poison to destroy cells directly, it functions as a highly targeted intelligence operation—training or modifying the host's own cytotoxic T cells to recognize, track, and eliminate the malignancy naturally.
[ THE IMMUNE CHECKPOINT INHIBITION LOOP ]
│
┌────────────────────────┴────────────────────────┐
▼ ▼
[ THE INFRARED CLOAKING MASK ] [ THE THERAPEUTIC UNMASKING ]
• Tumors overexpress PD-L1 surface proteins • Monoclonal antibodies bind to PD-1/PD-L1
• PD-L1 binds to T-cell PD-1 receptors • The molecular inhibitory signal is broken
• "Friend" signal sent; T-cell deactivates • T-cell pulls back cloak; destroys tumor
- Immune Checkpoint Inhibition (ICI): Cancer cells are highly adept at exploiting the immune system's natural safety valves to evade destruction. By overexpressing surface proteins like PD-L1, tumors bind directly to the PD-1 receptors on tracking T cells, sending an inhibitory signal that forces the immune cell to stand down. Modern checkpoint inhibitors use engineered monoclonal antibodies to block this pathway, stripping away the tumor's camouflage so the patient's immune system can execute its target mission.
- Adoptive Cell Transfer & CAR-T Engineering: At the cutting edge of cellular design, Chimeric Antigen Receptor (CAR) T-cell therapy involves harvesting a patient’s own immune cells, genetically modifying them in a laboratory to express synthetic receptors optimized to lock onto specific tumor markers, and re-infusing them as a living, self-replicating defense force.
- Next-Generation Modalities: Contemporary pipelines feature bispecific antibodies—engineered molecules that simultaneously bind to a tumor antigen and a T-cell receptor, mechanically dragging the body's immune defenses directly into contact with the malignancy.
Comparative Matrix: Broad Cytotoxicity vs. Targeted Immuno-Oncology
The matrix below contrasts the operational differences between chemotherapy's broad mitotic strategy and immunotherapy's precise biomolecular profiling framework.
|
Clinical Vector Matrix |
Conventional Cytotoxic Chemotherapy |
Advanced Precision Immunotherapy |
Strategic Last-Mile Advantage |
|---|---|---|---|
|
Primary Cellular Target |
Active cellular mitosis and rapid DNA replication loops. |
The host immune system's signaling networks. |
Protects non-dividing healthy tissues from collateral damage. |
|
Speed & Onset of Action |
Rapid tumor shrinkage typically visible within initial cycles. |
Slower initial response; immune networks take time to organize. |
Chemo remains critical for urgent debulking of aggressive masses. |
|
Durability of Response |
Transience; risk of rapid bounce-back once active dosing stops. |
Long-lasting protection via immunological memory. |
Generates years-long survival curves in responsive patients. |
|
Biomarker Dependency |
Minimal; prescribed based on broad histological staging. |
High dependency on NGS panels, PD-L1 expression, and MSI status. |
Eliminates therapeutic guesswork by matching treatment to tumor biology. |
|
Toxicity Profile |
Systemic: Alopecia, myelosuppression, and mucositis. |
Immune-related adverse events (e.g., colitis, pneumonitis). |
Shifts side-effect management from symptom control to auto-immune tracking. |
3. The Precision Synergy: Chemo-Immunotherapy
Modern precision oncology increasingly rejects an "either-or" paradigm. Instead, treatment sequencing frequently leverages a powerful clinical combination known as Chemo-Immunotherapy.
When chemotherapy runs its initial cycle, its rapid destruction of the main tumor mass causes immunogenic cell death. As the malignant cells rupture, they spill a massive wave of tumor-specific proteins (neoantigens) directly into the surrounding tissue. This cellular destruction serves as a powerful warning beacon for the body's defenses.
By administering checkpoint inhibitors alongside this cycle, oncologists can instantly train the newly alerted T cells to recognize the released antigens, creating a highly effective combination where chemotherapy opens the door and immunotherapy walks through it to clear out residual microscopic disease.
4. Operational Strategy: A Clinical Implementation Protocol
To safely integrate precision oncology platforms into modern healthcare infrastructure, institutional medical boards and clinical directors must follow a structured operational blueprint:
- Mandate Pre-Treatment Biomarker & Next-Generation Sequencing (NGS)
Phase 1
Dismantle traditional, unguided prescription habits. Before authorizing advanced systemic therapies, mandate the execution of a comprehensive molecular diagnostic panel to map the tumor's exact PD-L1 expression levels, Microsatellite Instability (MSI-High) status, and overall Tumor Mutational Burden (TMB), ensuring clear biological alignment. - Deploy Standardized Cross-Departmental Toxicity Workflows
Phase 2
Prepare front-line medical teams for the unique side-effect profile of immune therapies. Establish clear step-up clinical workflows, early monitoring systems, and rapid corticosteroid intervention pathways within your emergency and nursing stations to identify and manage immune-related adverse events like pneumonitis, colitis, or thyroid inflammation before they escalate. - Integrate Unified Digital Registries for Real-Time Response Auditing
Phase 3
Ditch delayed, manual paper tracking systems. Connect your clinic's electronic medical records natively with a secure digital database using unified health exchange frameworks, allowing the oncology board to audit treatment sequencing timelines, evaluate long-term survival curves, and optimize care pathways continuously.
Actionable Strategy: Your Institutional Governance Plan
- Incorporate Interoperable Digital Health ID Account Linking Natively: Ensure your facility's administrative desks leverage unified digital tracking platforms. Linking electronic charts natively via a patient's digital health ID preserves lifetime molecular diagnostics histories, prevents clinical data fragmentation, and eliminates redundant, costly genomic re-testing across separate network sites.
- Establish Routine Screening for Minimal Residual Disease (MRD): Maximize the power of precision monitoring by integrating ultra-sensitive liquid biopsies following active treatment cycles. Utilizing blood-borne circulating tumor DNA (ctDNA) fragmentomics allows your team to spot microscopic molecular recurrences months before a physical mass becomes visible on standard radiological CT scans.
- Conduct Semi-Annual Quality Audits on Combined Modality Sequencing: Bring your medical oncologists, radiation therapists, and laboratory directors together for a structured performance check. Review average timeline intervals between initial debulking chemotherapy and subsequent immunotherapy maintenance cycles to ensure workflows match international best-practice standards.
Frequently Asked Questions (FAQs)
Q1. Why does chemotherapy cause hair loss while immunotherapy typically does not?Chemotherapy acts as a broad cytotoxic agent that attacks any cell undergoing rapid division. Because hair follicle cells divide constantly to produce hair shafts, they are targeted along with the tumor. Immunotherapy does not affect cellular division mechanics directly; it modifies immune cell signaling receptors, leaving healthy hair replication completely undisturbed.
Q2. What exactly does a "High PD-L1 Expression" score mean on a molecular pathology report?PD-L1 is a specialized protective protein that cancer cells use as a visual camouflage to hide from immune surveillance by binding to T-cell PD-1 receptors. A high PD-L1 expression score indicates that the tumor is heavily reliant on this specific "hiding" mechanism, serving as a strong biological marker that the cancer will respond exceptionally well to checkpoint inhibitor drugs designed to block it.
Q3. How does "immunological memory" help prevent cancer from returning long after treatment ends?When immunotherapy unmasks a tumor, it prompts the patient's immune system to generate long-lived memory T cells. These specialized cells remain active within the bloodstream for years, maintaining a continuous surveillance loop that allows them to instantly recognize, intercept, and destroy the same cancer cells if they attempt to replicate in the future.
Q4. What are immune-related adverse events (irAEs), and why do they occur?Because immunotherapy works by taking the brakes off the body's immune system, the activated T cells can occasionally become overactive and mistake healthy tissue for foreign threats. This can trigger autoimmune-like inflammation in healthy organs, presenting clinically as pneumonitis (lung inflammation), colitis (colon inflammation), or hepatitis (liver inflammation).
Q5. What is the difference between a standard liquid biopsy and a traditional tissue biopsy?A traditional biopsy requires an invasive surgical procedure or needle extraction to harvest a physical piece of a tumor mass. A liquid biopsy requires only a simple blood draw, searching the plasma for floating fragments of cell-free DNA (cfDNA) shed by malignant cells to track tumor genetics and identify recurrences non-invasively.
Q6. Why is Microsatellite Instability (MSI-High) status a critical metric in precision oncology?Cancers with high microsatellite instability (MSI-High) possess a broken DNA mismatch repair system, which causes them to accumulate thousands of genetic mutations. All these mutations cause the cancer cells to look highly abnormal compared to healthy tissue, essentially painting a massive molecular target on the tumor that makes it highly vulnerable to immunotherapy.
Q7. How do bispecific antibodies optimize the immune system's target accuracy?Bispecific antibodies are dual-action engineered molecules equipped with two separate binding sites. One side attaches firmly to a specific antigen on the surface of the cancer cell, while the other side locks onto a receptor on a cytotoxic T cell, acting as a physical bridge that drags the immune cell straight into contact with its target.
Q8. Can a patient with an existing autoimmune disease safely receive checkpoint inhibitors?Prescribing checkpoint inhibitors to patients with pre-existing autoimmune diseases requires extreme clinical caution. Because these therapies unleash systemic immune activity, they carry a high risk of exacerbating the underlying autoimmune condition, requiring close oversight by a multi-disciplinary medical board.
Q9. Why does pancreatic cancer frequently demonstrate resistance to current immunotherapies?Pancreatic tumors are surrounded by a dense, unsupportive structure known as an immunosuppressive tumor microenvironment, often described as a "cold" tumor. This microenvironment acts as a physical and chemical shield that blocks T cells from entering the mass, making standard checkpoint inhibitors ineffective without combined synergistic therapies.
Q10. How long does it take to see a clinical response after transitioning to precision oncology workflows?While conventional chemotherapy shrinks high-volume masses rapidly within the initial weeks, precision immuno-oncology systems operate on an immunological timeline. By deploying advanced biomarker screening, matching drugs to tumor genetics, and utilizing automated monitoring dashboards, a clinic can observe stable molecular responses and improved patient tolerance profiles within 4 to 6 weeks of active system rollout.






.jpeg)
.jpg)
.jpg)
.jpg)
.jpeg)

.jpg)



.jpg)

.jpg)

